")
")
")
")
")
HOW VACCINE CAUSES MYO-PERICARDITIS
Intravenous Injection of Coronavirus Disease 2019 (COVID-19) mRNA Vaccine Can Induce Acute Myopericarditis in Mouse Model
Vaccine hesitancy among the general public is a significant problem and is partially driven by the apprehension of rare but potentially severe side effects of these rapidly developed novel vaccines. An example of such a side effect is myopericarditis following mRNA COVID-19 vaccines, which has a crude incidence of 40.6 cases per million second doses administered to males aged 12−29 years [4]. The pathogenesis of this unexpected complication remains elusive.
The World Health Organization (WHO) [5] and Centers for Disease Control and Prevention (CDC) [6] no longer recommend aspiration of syringe plunger during intramuscular injections, especially during vaccination when a rapid injection of a small volume may reduce discomfort. https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciab707/6353927
This study was published 18 August 2021. It provided us with reason to suspect that pericarditis occurs mostly in young men because they tend to have more muscles in their arms than women, thus more or larger blood vessels, thus greater chance for the needle to hit one.
One would have expected the WHO and CDC to publicise warning to nurses, to aspire syringe to see whether by chance they have not hit a blood vessel. Dr. John Campbell, on his September 26 2021 YouTube lecture, expressed anger about the fact that no warning had as yet come from the authorities.
Silence is the simplest conspiracy: to comply, we just look right, left, or behind. However, as agreed, we do not look at what's in front of our face. Was this a conspiracy to hide a possible solution to the problem afflicting thousands of young men? Not necessarily. It could also be ignorance or stupidity. Or shyness. The sensitive bullies who run the world fear making still more mistakes, they do not want to answer question. The easiest way to escape from answering is saying, "We are examining the situation. We'll advise you any changes."
Most likely, they fear slowing down the vaccination business. They want big smiles: "So fast! Didn't hurt at all! Can I come back soon for one more shot?" Retracting the syringe plunger would show that you hit a blood vessel. Then you would have to stick the needle in again, and retract again. That might hurt.
EXPONENTIAL GROWTH: 5/M - 300/M
AT CDC, A TRADITION OF GOOD DATA AND FAKE CONCLUSIONS
Optimistic statistics have been a problem since the Covid-19 vaccine trials of 2020.
"Bell’s palsy was reported by four vaccine recipients and none of the placebo recipients. The frequency of reported Bell’s palsy ["BP"] in the vaccine group is consistent with the background rate in the general population, and there is no basis upon which to conclude a causal relationship." https://www.cdc.gov/vaccines/covid-19/info-by-product/pfizer/reactogenicity.html
That was a false and deceptive report. A correct calculation would have showed a twenty-fold increase in BP cases over background rate in the general population. Miscalculation was used to hide reality from us.
Pfizer could not explain the mechanism by which their vaccine was causing damage. So they dared to deny the reality of damage with a little prestidigitation. https://www.covidr.org/en/85-three-cards-monte-to-hide-unpleasant-data-at-fda.
The doctors who administered the trials played fair, and did present the horrendous data to CDC and FDA: "Reports of lymphadenopathy were imbalanced with 58 more cases in the vaccine group (64) than the placebo group (6)"
Lymphadenopathy, however, was not seen as a serious adverse event. "The most common serious adverse events in the vaccine group which were numerically higher than in the placebo group were appendicitis (7 in vaccine vs 2 in placebo), acute myocardial infarction (3 vs 0), and cerebrovascular accident (3 vs 1). " https://www.cdc.gov/vaccines/covid-19/info-by-product/pfizer/reactogenicity.html
CDC and FDA mentioned the problems in their reports. They concluded that that the tripling of serious problems was none of their problem, since the vaccine was safe: it had to be safe, of course, since they could not figure how their blessed vaccine could have caused a three-fold increase in appendicitis, myocardial infarction, and cerebrovascular accident,
But they sure did not play fair when 12-year-old Maddie de Garay was paralyzed in the Pfizer trial, hours after the vaccine. They could not explain the event. So they decided it was none of their problem and just cancelled her. Viciously, they ignored her and her family's tragedy. By the way, when Senator Johnson brought Ms. Garay and her mother to a press conference, the national press pressed on, ignoring the event. Even the local papers and TV stations in Milwakee attacked the senator. That was one paralysis in 1200 vaccinees. Totally omitted from the happy statistics
In 2020, there was pressure to ignore bad news, in Washington as in Paris, in Tokyo as in Peking; we still see the same pressures in 2021. A self-evident conspiracy of silence could be observed in Peking, in January 2020. It's still noticeable in the world's media and in almost all governments. Reality, however, is beginning to make headway in poor countries, some large Indian states and some small European and South American states are distributing ivermectin.
LET'S MINIMIZE MYO-PERICARDITIS
The most reputable organisations have lied to us. Here are some good false news from the American Academy of Pediatrics: “The facts are clear: this is an extremely rare side effect, and only an exceedingly small number of people will experience it after vaccination. Importantly, for the young people who do, most cases are mild and individuals recover often on their own or with minimal treatment."
The statement above can only be described as murderous, or criminally insane. It would be excusable to say that to a poor kid who cannot run any more; to say it to encourage other kids into is vaccination is a criminal act. To minimise myo-pericarditis is reckless. When it results in more kids being damaged, having been forced into vaccination, ir is murderous act.
Trial Site News thus commented on the above AAP statement: “Myocarditis can be deadly and with life long catastrophe like heart failure in years to come, and the seeds sown now as heart muscle is known to scar with inflammation and not recover or regenerate etc. and the danger is the ‘silent’ myocarditis that can only be detected with troponin etc. and via some incidental finding; there is chest pain, heart failure, contractile problems, damage to the heart’s electrical properties etc. and the concern is that this sets the person up for future serious heart anomalies and possible death... recovery is often not complete” https://trialsitenews.com/the-lies-by-the-american-academy-of-pediatrics-aap-and-dr-fauci-on-myocarditis-risk-and-covid-19-delta-variants-how-many-lies-can-one-press-release-contain/
MYOCARDITIS GETS REAL POPULAR, FROM 5/M TO 300/M
EMA, the European Medicines Agency said on May 28 2021, that they had received 107 reports of myocarditis following the Pfizer-BioNTech vaccine, or about one in 175,000 doses administered, or 5 cases/M. Few young men had been vaccinated, at the time. In that way, the problem remained hidden. https://www.science.org/news/2021/06/israel-reports-link-between-rare-cases-heart-inflammation-and-covid-19-vaccination
Wikipedia, on October 1, still sees "very rare" myocarditis and pericarditis cases in young males, 13/million vaccinations, see citation below.
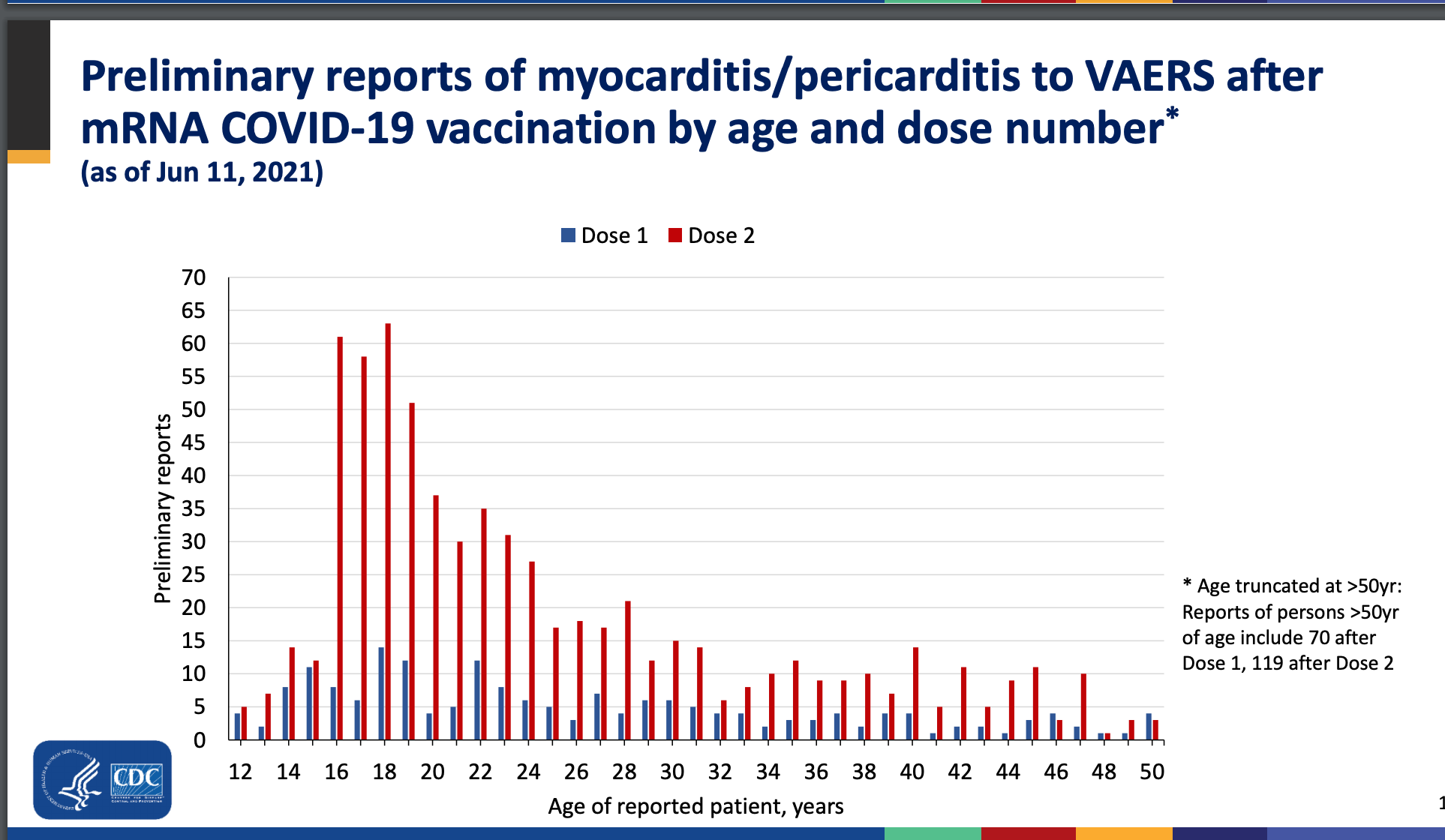
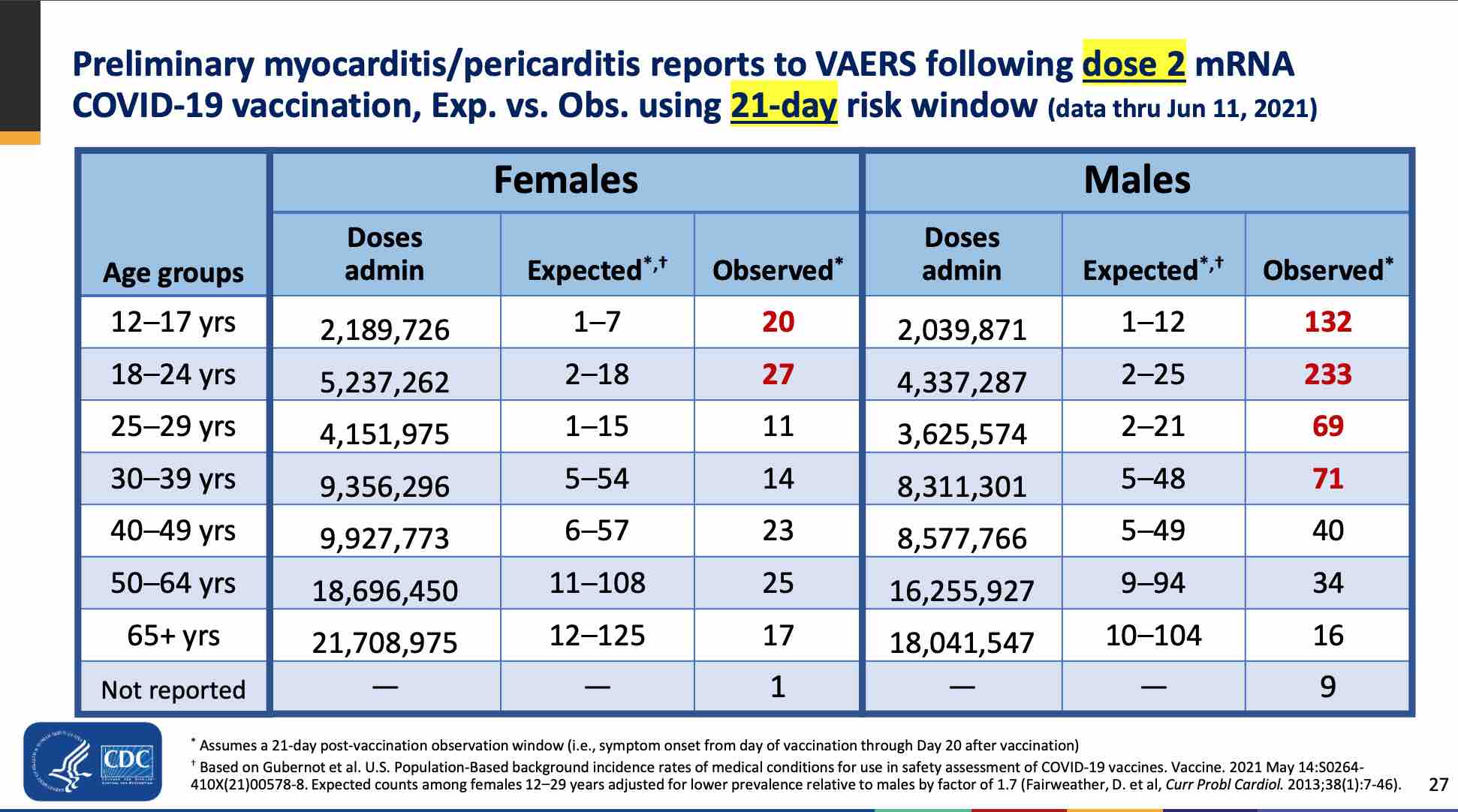
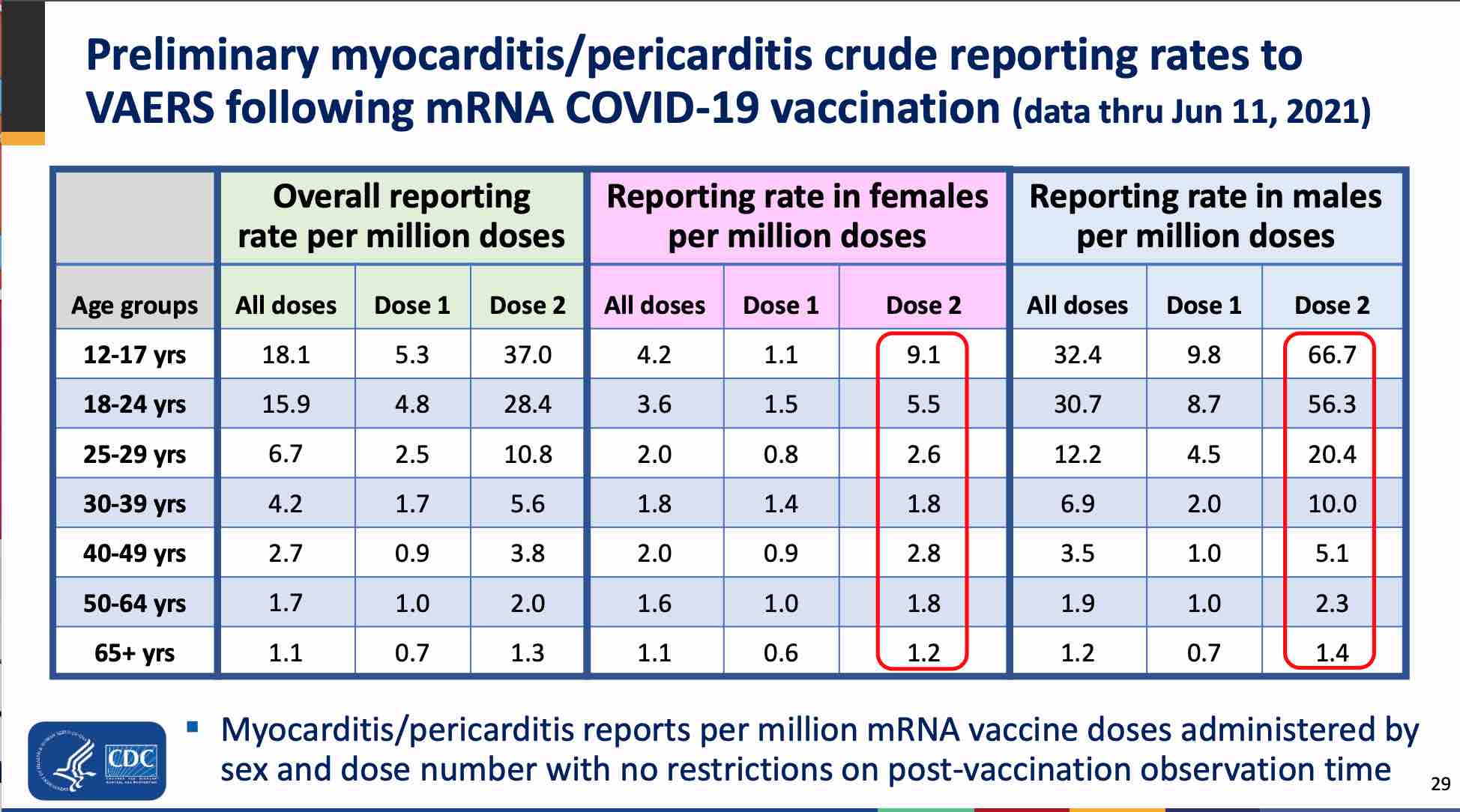
CDC, see charts below, finds 66 such rare cases/million vaccinations.
VAERS-based study comes up with 94 to 162 rare cases/million vaccinations, depending on patient's age.
According to Science, The COVID-19 vaccine made by Pfizer and BioNTech appears to put young men at elevated risk of developing a heart muscle inflammation called myocarditis, researchers in Israel say. In a report submitted today to the Israeli Ministry of Health, they conclude that between one in 3000 and one in 6000 men ages 16 to 24 who received the vaccine developed the rare condition. [that's 300-600/M] https://www.science.org/news/2021/06/israel-reports-link-between-rare-cases-heart-inflammation-and-covid-19-vaccination
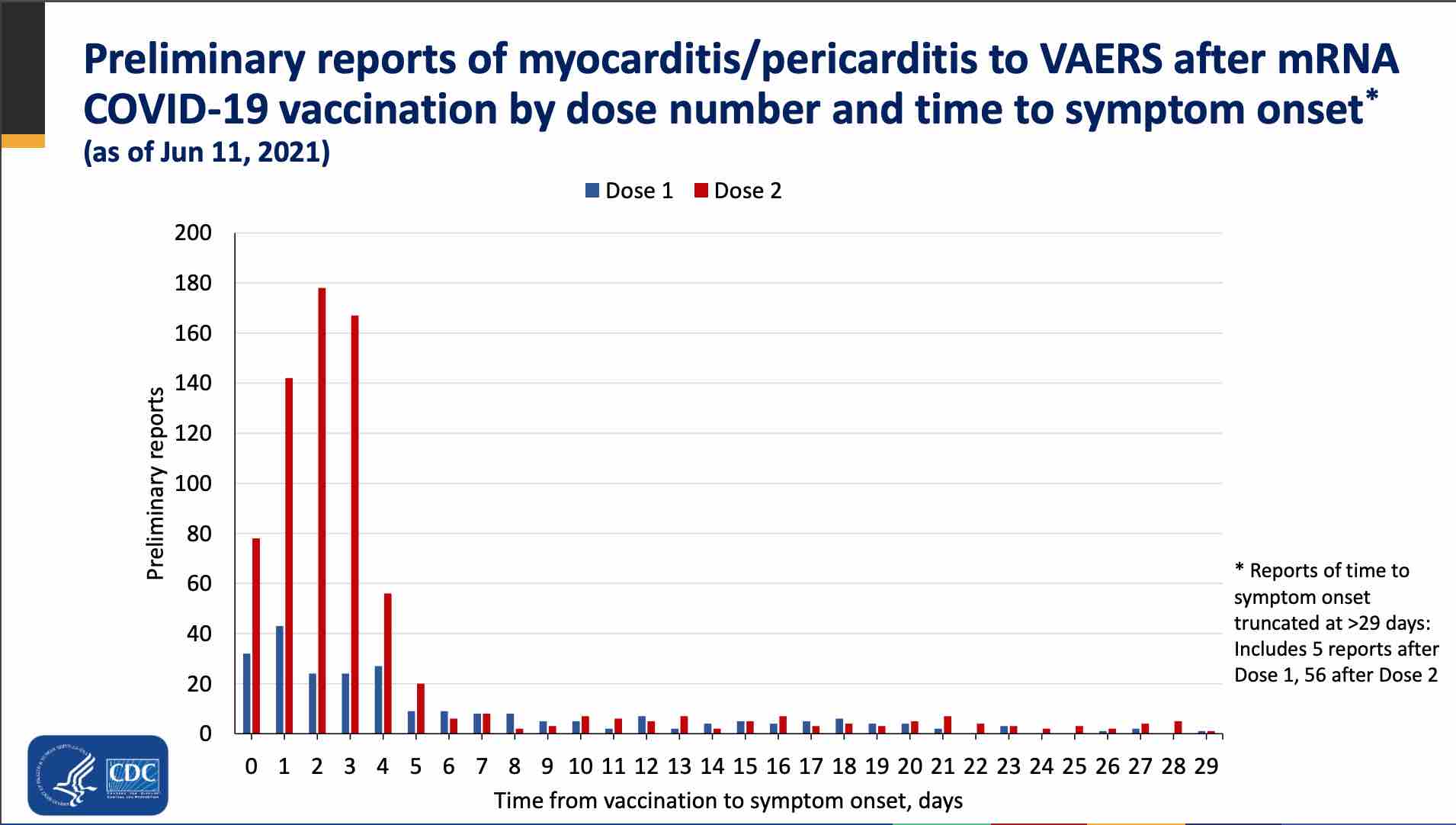
Dr. Dror Mevorach, who headed the national committee to investigate the myocarditis link, said that over a span of three months the hospital saw 20 cases of myocarditis, when it typically sees only four; 19 of the 20 cases were young males, ages 16 to 30. Eighteen of the 20 cases presented within four days of the second vaccine dose. The patients all had chest pain or difficulty breathing, ruling out that the condition was asymptomatic and caught inadvertently by general tests, Mevorach said. Only two patients of the 20 had evidence of past infection, eliminating any correlation with COVID-19 itself, rather than the vaccine. https://nymag.com/intelligencer/2021/06/israel-detects-link-between-myocarditis-and-covid-vaccine.html
"Anecdotal" is Dr. Fauci's preferred words. Yes, we must ignore a five-fold increase in illness until when Dr. Mevorach's eventual paper is published.
We must try to be understanding, be patient and wait, for our shepherds are too busy now, day-trading futures on our wool. "Wool production has been superlative this year, thank you. The product is of very high quality. The shearing is making progress everywhere. The herds in the tribal border areas are now being managed and corralled."
SARS-CoV-2 mRNA Vaccination-Associated Myocarditis in Children Ages 12-17: A Stratified National Database Analysis
Objectives Establishing the rate of post-vaccination cardiac myocarditis in the 12-15 and 16-17-year-old population in the context of their COVID-19 hospitalization risk is critical for developing a vaccination recommendation framework that balances harms with benefits for this patient demographic.study showed that cardiac events after vaccine are much more likely for young people, than hospitalisation due to covid-19.
Design, Setting and Participants Using the Vaccine Adverse Event Reporting System (VAERS), this retrospective epidemiological assessment reviewed reports filed between January 1, 2021, and June 18, 2021, among adolescents ages 12-17 who received mRNA vaccination against COVID-19. Symptom search criteria included the words chest pain, myocarditis, pericarditis and myopericarditis to identify children with evidence of cardiac injury. The word troponin was a required element in the laboratory findings. Inclusion criteria were aligned with the CDC working case definition for probable myocarditis. Stratified cardiac adverse event (CAE) rates were reported for age, sex and vaccination dose number. A harm-benefit analysis was conducted using existing literature on COVID-19-related hospitalization risks in this demographic.
Results A total of 257 CAEs were identified.
Rates per million following dose 2 among males were 162.2 (ages 12-15) and 94.0 (ages 16-17);
among females, rates were 13.0 and 13.4 per million, respectively. For boys 12-15 without medical comorbidities receiving their second mRNA vaccination dose, the rate of CAE is 3.7 to 6.1 times higher than their 120-day COVID-19 hospitalization risk as of August 21, 2021 (7-day hospitalizations 1.5/100k population) and 2.6-4.3-fold higher at times of high weekly hospitalization risk (7-day hospitalizations 2.1/100k), such as during January 2021.
For boys 16-17 without medical comorbidities, the rate of CAE is currently 2.1 to 3.5 times higher than their 120-day COVID-19 hospitalization risk, and 1.5 to 2.5 times higher at times of high weekly COVID-19 hospitalization. https://www.medrxiv.org/content/10.1101/2021.08.30.21262866v1
RAGE AGAINST BAD NEWS
The authors were , , , Dr. David Gorski breathlessly launched odd lengthy personal attacks on the four authors for sins of omission and commission:
From an exchange on a discussion board: Tracy Beth Hoeg, MD, PhD: This paper has no sponsorship nor any relationship to rational ground. I am the leading author and just had to look up what rational ground even was.
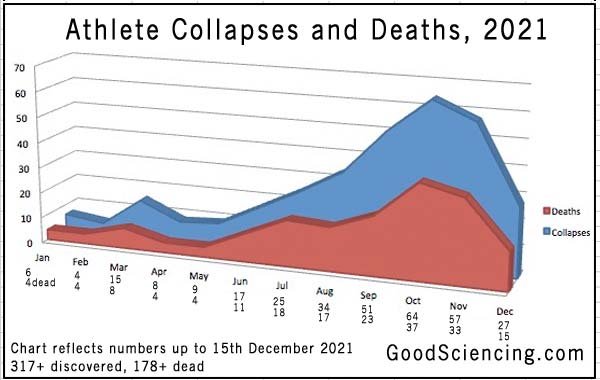
It is definitely not normal for young athletes to suffer from cardiac arrests or to die while playing their sport, but this year it is happening. All of these heart issues and deaths come shortly after they got a COVID vaccine. While it is possible this can happen to people who did not get a COVID vaccine, the sheer numbers clearly point to the only obvious cause...
Many sports teams now have multiple sidelined players. There are dozens of them. The teams and Big Media are hiding this, thinking nobody will notice. These damaged players will not be shown in this report if they are reported only as “illness” but they would be worth tracking, because it is not normal to have so many. Their immune systems are likely to have been compromised by “something,” so they will be open to many things they would normally have been able to shrug off. We leave it to others to track these – we have our hands full handling the investigations for this list, going back in time trying to find new information that wasn’t available before, and making minor corrections as they are discovered. It will all come out eventually.
Myocarditis, also known as inflammatory cardiomyopathy, is inflammation of the heart muscle. Symptoms can include shortness of breath, chest pain, decreased ability to exercise, and an irregular heartbeat.[1] The duration of problems can vary from hours to months. Complications may include heart failure due to dilated cardiomyopathy or cardiac arrest.[1].
Epidemiology
One notable instance of viral myocarditis is the involvement of the SARS-CoV-2 virus; fulminant myocarditis from cardiac damage and SARS-CoV-2 has been associated with high mortality rates.[44] Myocarditis can also, rarely, be caused by vaccination against Covid-19;[24][25] however, the risk of myocarditis due to vaccination is less than the risk of myocarditis following infection,[46] and far less than the risks of other harm due to infection.
To separate the hundreds of thousands of excess of heart conditions expected to arise in the UK from the covid vaccination, a new disorder has been announced, the PPSD, or Post Pandemic Stress Disorder. https://www.standard.co.uk/news/health/post-pandemic-stress-disorder-heart-conditions-covid-london-physicians-b969436.html
Myocardial injury is found among hospitalised covid patients.
According to a 2020 review, approximately 5%-25% of patients hospitalized with COVID-19 have had evidence of myocardial injury...The use of CMR led to a 7.4-fold increase in the detection of myocarditis cases; only 0.31% of cases would have been detected without CMR. [cardiac magnetic resonance imaging ] https://www.thecardiologyadvisor.com/general-cardiology/heart-inflammation-after-covid-19-infection-in-athletes/
If 99% of cases need CMR to be noticed, we must ask whether the cases of myocarditis-after-vaccine would be multiplied with CMR. It seems reckless to recommend a vaccination that leads to hospitalisation more often than Covid-19 among young people. Moreover, the risk of harm from infection is minimal in young people, and would be further minimized if prevention and cure were allowed.
Since a leaky vaccine campaign helps to develop deadlier variants, does not protect from Covid-19, and is effective for a few months only, rational people would try to wipe out covid, with vaccination + prevention: ivermectin, vitamin D, vitamin C, zinc, quercetin, following FLCCC protocols.
It is now impossible to extinguish Covid-19 with a vaccine, but it can be done with covid prophylaxis. In some Indian states such as Uttar Pradesh, they would be close to extinguish it with ivermectin, but in other states, corrupt politicians have been pressured to use remdesivir, which has no effect on Covid-19, but costs thousands.
COVID-19 vaccine clinical research From Wikipedia, the free encyclopedia. September 30, 2021
Side effects
|
This section needs expansion. You can help by adding to it. (July 2021)
|
Serious adverse events associated with receipt of new vaccines targeting COVID-19 are of high interest to the public.[618] All vaccines that are administered via intramuscular injection, including COVID-19 vaccines, have side effects related to the mild trauma associated with the procedure and introduction of a foreign substance into the body.[619] These include soreness, redness, rash, and inflammation at the injection site. Other common side effects include fatigue, headache, myalgia (muscle pain), and arthralgia (joint pain) which generally resolve within a few days.[620] One less-frequent side effect (that generally occurs in less than 1 in 1,000 people) is hypersensitivity (allergy) to one or more of the vaccine's ingredients, which in some rare cases may cause anaphylaxis.[621][622][623][624] More serious side effects are very rare because a vaccine would not be approved even for emergency use if it had any known frequent serious adverse effects.
We ask about the thousands of healthy people who died within hours of the jab. They answer inanities about sore shoulders.
Then, the best of all possible answers: "It's safe, because it's approved." In this best of all possible world, Wikieditors are true believers.
To resist cognitive dissonance, they miss all data in conflict with the vaccinal cult's tenets. It's comfortable to miss the data, it relieves one of anger and fear. Wikieditors have joined a scientific Taleban, always ready with perfect data; thus they have no need for data from infidels.
How can Wikieditors defend their beliefs from studies like the ones presented above? They repeat the mantra "unreliable VAERS." It is the only collection of data they allow, yet they do not want us to use them because they are incomplete. They do not want to know the consequence of what the pharma oligarchy has imposed on us.
Embolic and thrombotic events
The Janssen COVID-19 vaccine reported rare formation of blood clots in the blood vessels in combination with low levels of blood platelets known as thrombosis with thrombocytopenia syndrome (TTS) which occurred at a rate of about 7 per 1 million vaccinated women ages 18–49 years old; and even more rarely for other populations.[615]
According to the CDC, very rare cases of myocarditis and pericarditis have been reported in the United States, in about 13 per million young people (mostly in males and mostly over the age of 16), after vaccination with the Pfizer–BioNTech's or Moderna's vaccines.[616] According to reports, the recovery from these rare side effects is quick in most individuals, following adequate treatment and rest.[617]
13/million? Yet, the chart presented by CDC gives us 66/M, not 13/M. From the University of Ottawa study, we learn that the rate is 1/1000, or 1000/M
Looking at indicated notes, [616] [617] we do not find the silly 13/M claim.
Perhaps, to hide the catastrophic teenagers' results, to mask the awful results for 17-19-year-olds, did someone blend the 17-19 data into the 16-30-year-olds category?